Heart burn, acid reflux, GERD – what is the difference?
All of these conditions occur when acid from the stomach escapes into your oesophagus, via the sphincter at the top of the stomach, creating a burning sensation.
All of these painful digestive conditions are related and tend to cause similar symptoms, however, they usually develop in stages.
In the case of acid reflux, stomach acid leaks out of the stomach and into the oesophagus. When this progresses, it can be diagnosed as gastroesophageal reflux disease (GERD) which is considered to be more severe. Heartburn is also commonly called GERD.
The most common symptom of GERD is frequent pains in the chest and burning sensations hence the name “heartburn”. Other signs of GERD are difficulty swallowing or keeping down food and liquids, coughing, wheezing and chest pain. Often these symptoms occur or are much worse at night.
An alarming finding from one study conducted in Norway found that the incidence of acid reflux rose from around 11 percent of the population to over 17 percent over a period of 11 years. A similar rise is happening in other industrialised countries too.
It might not be the biggest deal to have acid reflux symptoms on occasion but research shows that people with long-standing, chronic heartburn are at greater risk for serious complications. These include stricture (narrowing) of the oesophagus and inflammation of the oesophagus or oesophagitis. Other developments can include chronic infections and there are concerns re fracture risk and pneumonia (linked to PPI medication).
If we have low stomach acid our food isn’t broken down as quickly or completely so proteins stay in the stomach longer than is normal. This means the acid also stays longer and this can cause digestive issues, especially when we start moving around following a meal. Slowing our digestion down is also a problem as it gives food time to ferment and putrification can occur. This means bacterial balance can become problematic as certain undesirable species thrive (pathogenic) and yeast and fungus can also start to proliferate. This in turn can lead to more serious problems from an unhealthy microbiome balance and conditions such as IBS and multiple digestive issues.
So we need our stomach acid but we need it in the right place.
Nutritional support for post-surgery
I frequently support clients who have either had or are going to have operations.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
I have recently been researching this area for a client with impending surgery This blog is focused on protein and carbohydrate requirements post operation. I will consider micronutrient status in a future blog.
Some degree of muscle loss post-surgery is inevitable. Skeletal muscle serves as the primary source of essential amino acids. If protein intake is below the requirement to sustain daily functions the body will breakdown muscle for protein. To compound this the hormonal stress response following surgery can prevent normal protein generation. All of this is often complicated further by the forced rest and immobility due to the surgery itself.
It is important to try to minimise the muscle loss and if exercise is not feasible nutritional strategies can help to mitigate this. In healthy individuals, loss of muscle tissue begins to occur in as little as 48 h of inactivity, with significant loss within five days. This is followed by loss of strength and functionality.
Post-surgical amino acid supplementation has been shown to effectively reduce the turnover of whole-body protein and muscle breakdown, and to stimulate an increase in protein generation.
General guidelines for nutrition post surgery
The goal of post-operative nutrition, on the other hand, is to promote nitrogen balance, reduce the loss of lean muscle mass, and facilitate rapid healing and recovery. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
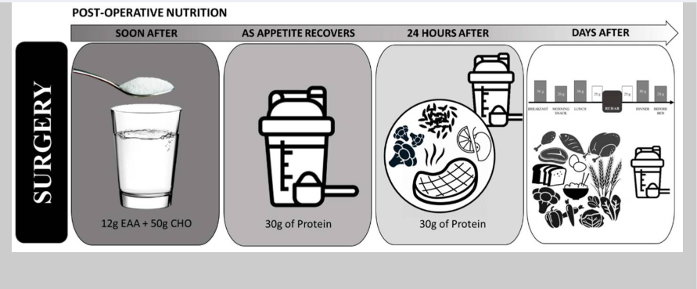
The post operative nutrition model is basically the reverse of the preoperative model.
In the early post-surgery period, patient appetite is often suppressed making consumption of solid foods difficult. During this time, free form EAA’s may help to support the immune system. Patients can transition to protein shakes and sports drinks until they are able to consume whole food sources or meals.
During the rehabilitation period, protein intakes of at least 1.6 g/kg/day and up to 2.0–3.0 g/kg/day is generally recommended. If appetite is reduced and this goal is difficult to meet then consumption of EAA’s and/or protein shakes between meals can help to optimise protein and nutrient intake.
Conclusion
In conclusion protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Following surgery, free form amino acids plus supplementary dietary protein can help to support protein generation and an increase in whole-body protein. Depending on proximity to surgery different sources of protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs post-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for or recover from planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
I frequently support clients who have either had or are going to have operations.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
I have recently been researching this area for a client with impending surgery This blog is focused on protein and carbohydrate requirements pre-operation. I will consider micronutrient status in a future blog.
Surgery is stressful and our energy demands increase. To cope with this our sugar stores (glycogen) are rapidly burnt from the liver and muscle. This can lead to significant skeletal muscles loss and some degree of this post-surgery is inevitable.
There some easy strategies you can implement though to help with muscle preservation and to support and accelerate healing. Carbohydrate consumption pre-operation helps to:
Support increased energy demand during the initial period and to cope with the initial inflammatory state.
Reduce muscle wastage and preserve lean body mass.
Manage the insulin resistance which is common post-surgery. Remember insulin resistance will prevent glucose entering your cells. This is important because the body will generate its own glucose (gluconeogenesis) due to the stress and it is important that the cells can absorb this.
General guidelines for nutrition before surgery
The goal is to prepare the body for the stress of surgery, support increased metabolic demand, whilst offsetting the consequences of the breakdown of body protein. The goal of pre-operative nutrition is to ensure adequate energy stores to meet the demands of the stress state. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
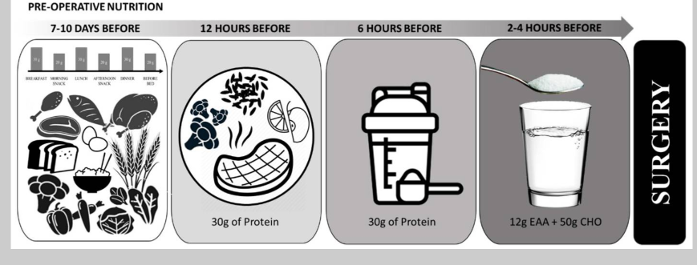
7-10 days prior to surgery - emphasise high-quality carbohydrate and protein intake to ensure optimal nourishment. To maximise glycogen stores, the sports nutrition model suggests consuming ~60% of total energy (8 g per kg body mass) per day of carbohydrate for a minimum of 3–4 days. Protein intakes of 1.2–2.0 g/kg/day, from high-quality protein sources distributed throughout the day (20–40 g of protein per meal) is recommended to help ensure protein needs are met.
6-12 hours before surgery – consume a well-rounded meal emphasising complex carbohydrates and high-quality protein.
6 hours before - begin abstaining from whole foods, but continue to consume protein and carbohydrate containing beverages, such as a protein shake, a sports drink, or chocolate milk. Since modified carbohydrate supplements rapidly empty from the stomach, consumption may sustain glucose levels for the duration of surgery.
2-4 hours before – It is suggested to ingest free form essential amino acids (EAA’s) to promote a positive protein balance. EAA’s contain all nine essential amino acids and do not require digestion.
Conclusion
In conclusion carbohydrate intake supports the increased post-surgical metabolic (energy) demand and wound healing. Protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Combined amino acid and glucose intake can help to mitigate muscle loss and strength, especially prior to surgery. Depending on proximity to surgery different sources of carbohydrate and protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs pre-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
Having surgery? Here are your nutrition guidelines.
I frequently support clients who have either had or are going to have surgery of various kinds.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
The biggest issues are muscle loss due to tissue breakdown and metabolic demand exceeding supply due to the increase in stress and energetic demand. Micronutrient status is also important but will be covered in a separate blog. This article is focused on protein and carbohydrate requirements both pre and post operation.
There some easy strategies you can implement to help with muscle preservation and to support and accelerate healing. Carbohydrate consumption pre-operation helps to:
Support increased energy demand during the initial period and to cope with the initial inflammatory state.
Reduce muscle wastage and preserve lean body mass.
Manage the insulin resistance which is common post-surgery. Remember insulin resistance will prevent glucose entering your cells. This is important because the body will generate its own glucose (gluconeogenesis) due to the stress and it is important that the cells can absorb this.
Post-surgical amino acid supplementation has been shown to effectively reduce the turnover of whole-body protein and muscle breakdown, and to stimulate an increase in protein generation.
General guidelines for nutrition before and after
Pre-Operative Nutrition
The goal is to prepare the body for the stress of surgery, support increased metabolic demand, whilst offsetting the consequences of the breakdown of body protein. The goal of pre-operative nutrition is to ensure adequate energy stores to meet the demands of the stress state. The goal of post-operative nutrition, on the other hand, is to promote nitrogen balance, reduce the loss of lean muscle mass, and facilitate rapid healing and recovery. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
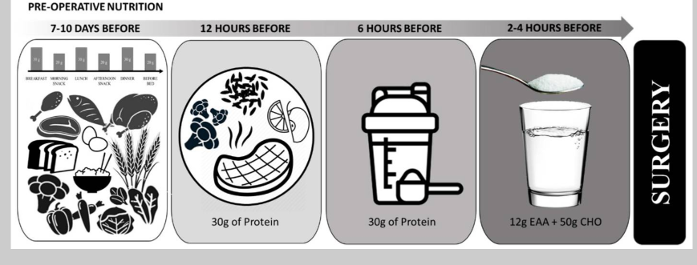
7-10 days prior to surgery - emphasise high-quality carbohydrate and protein intake to ensure optimal nourishment. To maximise glycogen stores, the sports nutrition model suggests consuming ~60% of total energy (8 g per kg body mass) per day of carbohydrate for a minimum of 3–4 days. Protein intakes of 1.2–2.0 g/kg/day, from high-quality protein sources distributed throughout the day (20–40 g of protein per meal) is recommended to help ensure protein needs are met.
6-12 hours before surgery – consume a well-rounded meal emphasising complex carbohydrates and high-quality protein.
6 hours before - begin abstaining from whole foods, but continue to consume protein and carbohydrate containing beverages, such as a protein shake, a sports drink, or chocolate milk. Since modified carbohydrate supplements rapidly empty from the stomach, consumption may sustain glucose levels for the duration of surgery.
2-4 hours before – It is suggested to ingest free form essential amino acids (EAA’s) to promote a positive protein balance. EAA’s contain all nine essential amino acids and do not require digestion.
Post-Operative Nutrition
The post operative nutrition model is basically the reverse of the preoperative model.
In the early post-surgery period, patient appetite is often suppressed making consumption of solid foods difficult. During this time, free form EAA’s may help to support the immune system. Patients can transition to protein shakes and sports drinks until they are able to consume whole food sources or meals.
During the rehabilitation period, protein intakes of at least 1.6 g/kg/day and up to 2.0–3.0 g/kg/day is generally recommended. If appetite is reduced and this goal is difficult to meet then consumption of EAA’s and/or protein shakes between meals can help to optimise protein and nutrient intake.
Conclusion
In conclusion carbohydrate intake supports the increased post-surgical energy demand and wound healing. Protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Combined amino acid and glucose intake can help to mitigate muscle loss and strength, especially prior to surgery. Following surgery, free form amino acids plus supplementary dietary protein can help to support protein generation and an increase in whole-body protein. Depending on the proximity to surgery different sources of carbohydrate and protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs both pre and post-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
I frequently support clients who have either had or are going to have operations.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
I have recently been researching this area for a client with impending surgery This blog is focused on protein and carbohydrate requirements both pre and post operation. I will consider micronutrient status in a future blog.
Surgery is stressful and our energy demands increase. To cope with this our sugar stores (glycogen) are rapidly burnt from the liver and muscle. This can lead to significant skeletal muscles loss and some degree of this post-surgery is inevitable. Skeletal muscle serves as the primary source of essential amino acids. If protein intake is below the requirement to sustain daily functions the body will breakdown muscle for protein. Despite this however, the hormonal stress response prevents normal protein generation. All of this is often compounded by the forced rest and immobility due to the surgery itself.
It is important to try to minimise the muscle loss and if exercise is not feasible nutritional strategies can help to mitigate this. In healthy individuals, loss of muscle tissue begins to occur in as little as 48 h of inactivity, with significant loss within five days. This is followed by loss of strength and functionality.
There some easy strategies you can implement though to help with muscle preservation and to support and accelerate healing. Carbohydrate consumption pre-operation helps to:
Support increased energy demand during the initial period and to cope with the initial inflammatory state.
Reduce muscle wastage and preserve lean body mass.
Manage the insulin resistance which is common post-surgery. Remember insulin resistance will prevent glucose entering your cells. This is important because the body will generate its own glucose (gluconeogenesis) due to the stress and it is important that the cells can absorb this.
Post-surgical amino acid supplementation has been shown to effectively reduce the turnover of whole-body protein and muscle breakdown, and to stimulate an increase in protein generation.
General guidelines for nutrition before and after surgery
Pre-Operative Nutrition
The goal is to prepare the body for the stress of surgery, support increased metabolic demand, whilst offsetting the consequences of the breakdown of body protein. The goal of pre-operative nutrition is to ensure adequate energy stores to meet the demands of the stress state. The goal of post-operative nutrition, on the other hand, is to promote nitrogen balance, reduce the loss of lean muscle mass, and facilitate rapid healing and recovery. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
7-10 days prior to surgery - emphasise high-quality carbohydrate and protein intake to ensure optimal nourishment. To maximise glycogen stores, the sports nutrition model suggests consuming ~60% of total energy (8 g per kg body mass) per day of carbohydrate for a minimum of 3–4 days. Protein intakes of 1.2–2.0 g/kg/day, from high-quality protein sources distributed throughout the day (20–40 g of protein per meal) is recommended to help ensure protein needs are met.
6-12 hours before surgery – consume a well-rounded meal emphasising complex carbohydrates and high-quality protein.
6 hours before - begin abstaining from whole foods, but continue to consume protein and carbohydrate containing beverages, such as a protein shake, a sports drink, or chocolate milk. Since modified carbohydrate supplements rapidly empty from the stomach, consumption may sustain glucose levels for the duration of surgery.
2-4 hours before – It is suggested to ingest free form essential amino acids (EAA’s) to promote a positive protein balance. EAA’s contain all nine essential amino acids and do not require digestion.
Post-Operative Nutrition
The post operative nutrition model is basically the reverse of the preoperative model.
In the early post-surgery period, patient appetite is often suppressed making consumption of solid foods difficult. During this time, free form EAA’s may help to support the immune system. Patients can transition to protein shakes and sports drinks until they are able to consume whole food sources or meals.
During the rehabilitation period, protein intakes of at least 1.6 g/kg/day and up to 2.0–3.0 g/kg/day is generally recommended. If appetite is reduced and this goal is difficult to meet then consumption of EAA’s and/or protein shakes between meals can help to optimise protein and nutrient intake.
Conclusion
In conclusion carbohydrate intake supports the increased post-surgical metabolic (energy) demand and wound healing. Protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Combined amino acid and glucose intake can help to mitigate muscle loss and strength, especially prior to surgery. Following surgery, free form amino acids plus supplementary dietary protein can help to support protein generation and an increase in whole-body protein. Depending on proximity to surgery different sources of CHO and protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs both pre and post-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
There is quite a long list of symptoms that may be related to or caused by low stomach acid. Just because you have these symptoms doesn’t necessarily mean low stomach acid is the issue. Some of these symptoms can be caused by other factors. But it is worth investigating and considering or discussing with your health practitioner to see what they think.
This is not an exhaustive list but some of the most common acid reflux and GERD symptoms include the following.
Symptoms that may mean you have low stomach acid:
Heartburn
Waking up in the middle of the night feeling like you’re choking or coughing
Dry mouth
Bad breath
Regurgitation of acidic foods
Bloating after meals and during bouts of symptoms
Nausea
Belching, gassiness, burping and flatulence after meals
Increased discomfort when bending over or lying down
Hoarseness upon waking or throughout the day
Chronic throat irritation, soreness and dryness
Hiccups that are difficult to stop
Bitter taste in your mouth, periodically or (for some people) throughout the day (some people taste regurgitated food or sour liquid at the back of their mouths/throats)
Gum irritation, including tenderness and bleeding
Bloody vomiting (possible sign of damage in the lining of the oesophagus)
Black stools
Difficulty swallowing (a possible sign of narrowing oesophagus)
Unexpected weight loss
Food intolerances
Many of these symptoms are downstream effects where the root cause can be traced back to low stomach acid or issues with digestive function. Over time they can build up as one symptom can lead to another and so on. Everything in the body is designed to work in sync. So one thing goes out of balance there is a kind of knock on effect on many other systems in the body.
Unfortunately, it’s not always as simple as just rectifying the stomach acid levels, as once people start to experience reflux this can cause very distressing painful symptoms. It needs a kind of targeted approach working on many different areas with different strategies and specific supplements. I will put together a top ten list to help you get started so look out for this.
Understanding stomach acid – it's role in digestion and health
Here’s a quick summary of some of the key functions of our stomach acid.
Breaksdown our food and activates many other digestive functions.
Controls microbial overgrowth and keeps gut bacteria in balance, preventing infection and acid reflux.
Controls fungal and yeast overgrowth such as candida.
Helps with micronutrient absorption especially B12.
Needed to stimulate bile production for the absorption of fats and for detoxification.
Stomach acid (HCL) also known as gastric acid is a hydrochloric acid solution. Your stomach produces about 4 litres a day and it performs a vital role for food digestion. Major functions include the following:
Controls food passage through the stomach
The lower oesophageal sphincter (LES) prevents the backflow of stomach acid into the oesophagus. The pyloric sphincter at the bottom of the stomach opens when food is ready to move into the small intestine for the next stage of digestion. Food entry and exit from the stomach is controlled by these sphincters which act like little gates. The pH of the stomach is controlled via stomach acid levels and this influences internal pressure to trigger them to open or close.
Digestion and absorption of food and nutrients
Our stomach acid directly acts on our food to break it down but it also activates enzymes to digest it further. This includes an enzyme called pepsin for protein digestion. Stomach acid also helps the body to absorb micronutrients such as vitamin B12, calcium, magnesium, zinc, copper, iron, selenium and boron.
Sterilises food and the gut
Most bacteria do not like acid so if they gain entry (via food) they are usually destroyed by the acidity. It also takes care of the majority of pathogens. This means it is very protective from infections of all kinds and helps to prevent an overgrowth of harmful bacteria (dysbiosis). The latter can lead to all sorts of digestive issues including gas, constipation, bloating, nausea and diarrhoea.
The presence of bacteria in the wrong location and resulting gas build up can exert pressure on the sphincter at the top of the stomach. If this opens at unwanted times the acid can leak into unprotected areas (acid reflux), which can cause tissue damage. The conundrum is that whilst we take medication to reduce stomach acid and symptoms such as heart burn, the initial problem, dysbiosis and gas, is facilitated by far too low levels of stomach acidity.
Digesting fats and detoxification
Low levels or absent stomach acid inhibit the liver from releasing bile which we need to digest and absorb our fats. A lack of proper bile flow will also inhibit our detoxification system and the excretion of toxins from the body. Stomach acid is therefore essential for detoxification.
Acid reflux and PPI’s
I help many of my clients to tackle their acid reflux which is a common and distressing complaint. It is estimated that 20% of Europe’s population suffer with this condition.
Acid reflux symptoms
Acid reflux occurs when the muscle at the top of the stomach weakened and acid from the stomach leaks into the oesophagus. There are a variety of symptoms which may be related to this common problem.
Common
Less common
Heartburn
Voice changes
Chest pain
Hoarseness
Dry cough
Sore throat
Nausea
Difficulty breathing – asthma symptoms
Thick and bubbly saliva
Teeth damage
Pain in the upper part of the abdomen
Damage to mucous membranes in the mouth
Lump in throat
PPI medication
Proton pump inhibitor medication such as omeprazole and iansoprazole reduce the production of stomach acid. They work by blocking an enzyme known as the ‘proton pump’ which is key for acid production, hence their name ‘proton pump inhibitors’ or PPI’s. They can reduce the acidity of the stomach by up to 90% and this can help to reduce the risk of stomach acid causing damage to the delicate windpipe (oesophagus)and reduce uncomfortable symptoms such as reflux, heart burn and indigestion.
PPIs are commonly used for conditions like gastroesophageal reflux disease (GERD), reflux and to reduce ulcer irritation. In 2019 over 60 million doses of the two most common PPI drugs were prescribed.
Problems with medication and low levels of stomach acid
Acid suppression medications are generally intended for short term use to help with immediate symptom relief which is often essential. Slowing down digestion however can cause undesirable side effects. People sometimes feel sick or become constipated whilst others may experience diarrhoea, abdominal pain and gassy bloating. The gut microbiome which is crucial for health can become very unbalanced, known as dysbiosis, and this can lead to small intestine bacterial overgrowth (SIBO). This is when the bacteria from the large intestine (colon) overgrow into the small intestine.
There is also a risk of bacteria migrating elsewhere in the body, such as the lungs, increasing the risk for pneumonia. The negative effects on digestion have also raised concern about reduced nutrient absorption and even an increased risk of fracture.
The solution
Simple diet and lifestyle changes may be all that is required. These might include losing weight, avoiding eating just before sleep or avoiding key food triggers such as alcohol, caffeine, spices and chocolate. Sometimes we need to work on improving the digestive capacity and healing the gut first, to really resolve matters. There are also some key supplements that can coat the interior of the GI tract to protect and nourish the cellular lining. It just depends how severe the problem is.
My approach
My approach works on the root cause of the problem and is tried and tested to address both symptoms and long-term solutions. To discuss your unique health concerns please get in touch for a free chat or book a call with me via my website.
References
Eom, C-S. et al. (2011) Use of acid-suppressive drugs and risk of pneumonia: a systematic review and meta-anlaysis. Canadian Medical Association Journal; 183(3) pp.310-319. doi: 10.1503/cmaj.092129
Cai, D., Feng, W. and Jiang, Q. (2015) Acid-suppressive medications and risk of fracture: an updated meta-analysis. International Journal of Clinical Experimental Medicine; 8(6); pp. 8893-8904. PMID: 26309543
What do Nutritional Therapists help with and how to find one?
You might be someone who gets bloated after every meal. Or someone who feels exhausted by mid-morning despite a full night’s sleep. Maybe your skin flares up regularly, or you’re dealing with unpredictable mood or energy changes.
These are just a few of the reasons people turn to nutritional therapists.
Common concerns supported by nutritional therapists include:
Digestive issues (IBS, bloating, reflux, gall bladder issues, gout etc.)
Fatigue or low energy
Pre diabetes and heart health especially cholesterol
Osteoporosis and issues with bone density
Skin conditions
Female hormonal health (PMS, perimenopause, PCOS)
Stress and mental wellbeing
Autoimmune conditions such as arthritis
Healthy ageing and preventive healthcare
Optimising athletic performance
You don’t need to be diagnosed with a condition to work with a nutritional therapist. Many clients seek support for prevention, performance, or simply to understand their bodies better.
Why People Seek Nutritional Therapy
Many people turn to nutritional therapists after trying multiple solutions—diets, supplements, or private testing—without clarity or consistent results. Others feel dismissed by standard medical care or overwhelmed by conflicting online advice.
Nutritional therapy offers a structured, evidence-informed approach to identifying patterns and making progress that lasts.
It’s ideal for anyone who:
Has symptoms that don’t have a clear medical diagnosis
Feels like they’ve tried everything but still don’t feel well
Wants to optimise health before issues become problems
Prefers natural, lifestyle-based strategies alongside medical care
How to Find a Qualified Nutritional Therapist
To ensure you’re working with a properly trained practitioner:
Look for CNHC registration – this confirms they are qualified and regulated
Check for BANT membership – this indicates high standards of ethics, education, and science-led practice
Discover the Value of Working with a BANT-Registered Nutritional Therapist
Nutritional therapists play a vital role in bridging the gap between general wellness advice and personalised healthcare. They take time to understand how your diet, genetics, environment, and lifestyle interact and use that insight to guide tailored, evidence-based recommendations that help you feel better, for longer.
Generic nutrition tips and one-size-fits-all plans can fall short. Working with a Registered Nutritional Therapist puts your individual needs at the centre. For many clients, it’s the first time their symptoms, history, and goals have been fully explored and connected into a clear plan.
This approach supports symptom improvement while also helping you reconnect with your body, increase daily energy, and take charge of your long-term wellbeing.
If you’re ready to stop guessing and start understanding what your body really needs, a Registered Nutritional Therapist could make all the difference. Please feel free to get in touch or book a call via my website.
What qualification dose a Nutritional Therapist have? Are they different from a "nutrionist"?
In the UK anyone can call themselves a “nutritionist”. The title is not legally protected so regardless of training anyone can call themselves a “nutritionist”.
However, Registered Nutritional Therapists including me are:
Fully trained in nutrition science and functional medicine
Required to register with the Complementary and Natural Healthcare Council (CNHC), a PSA-accredited regulatory body
Members of professional organisations like BANT (British Association for Nutrition and Lifestyle Medicine)
Required to follow a strict code of ethics and maintain Continuing Professional Development (CPD)
This level of regulation ensures clients are receiving safe, evidence-based advice from a qualified professional.It’s important to remember that only those registered with CNHC are recognised to deliver one-to-one clinical care.
In my case I trained with the Institute of Optimum Nutrition (ION) in London and gained a diploma (DipION, Distinction). I also did some preliminary training at the University of Westminster.