Heart burn, acid reflux, GERD – what is the difference?
All of these conditions occur when acid from the stomach escapes into your oesophagus, via the sphincter at the top of the stomach, creating a burning sensation.
All of these painful digestive conditions are related and tend to cause similar symptoms, however, they usually develop in stages.
In the case of acid reflux, stomach acid leaks out of the stomach and into the oesophagus. When this progresses, it can be diagnosed as gastroesophageal reflux disease (GERD) which is considered to be more severe. Heartburn is also commonly called GERD.
The most common symptom of GERD is frequent pains in the chest and burning sensations hence the name “heartburn”. Other signs of GERD are difficulty swallowing or keeping down food and liquids, coughing, wheezing and chest pain. Often these symptoms occur or are much worse at night.
An alarming finding from one study conducted in Norway found that the incidence of acid reflux rose from around 11 percent of the population to over 17 percent over a period of 11 years. A similar rise is happening in other industrialised countries too.
It might not be the biggest deal to have acid reflux symptoms on occasion but research shows that people with long-standing, chronic heartburn are at greater risk for serious complications. These include stricture (narrowing) of the oesophagus and inflammation of the oesophagus or oesophagitis. Other developments can include chronic infections and there are concerns re fracture risk and pneumonia (linked to PPI medication).
If we have low stomach acid our food isn’t broken down as quickly or completely so proteins stay in the stomach longer than is normal. This means the acid also stays longer and this can cause digestive issues, especially when we start moving around following a meal. Slowing our digestion down is also a problem as it gives food time to ferment and putrification can occur. This means bacterial balance can become problematic as certain undesirable species thrive (pathogenic) and yeast and fungus can also start to proliferate. This in turn can lead to more serious problems from an unhealthy microbiome balance and conditions such as IBS and multiple digestive issues.
Nutritional therapy can really help to support and often resolve this condition. It's best to work with a BANT qualified nutritionist. Do get in touch if you would like to understand more about how I work with this condition or if you have any questions.
So we need our stomach acid but we need it in the right place.
Having surgery? Here are your nutrition guidelines.
I frequently support clients who have either had or are going to have surgery of various kinds.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
The biggest issues are muscle loss due to tissue breakdown and metabolic demand exceeding supply due to the increase in stress and energetic demand. Micronutrient status is also important but will be covered in a separate blog. This article is focused on protein and carbohydrate requirements both pre and post operation.
There some easy strategies you can implement to help with muscle preservation and to support and accelerate healing. Carbohydrate consumption pre-operation helps to:
Support increased energy demand during the initial period and to cope with the initial inflammatory state.
Reduce muscle wastage and preserve lean body mass.
Manage the insulin resistance which is common post-surgery. Remember insulin resistance will prevent glucose entering your cells. This is important because the body will generate its own glucose (gluconeogenesis) due to the stress and it is important that the cells can absorb this.
Post-surgical amino acid supplementation has been shown to effectively reduce the turnover of whole-body protein and muscle breakdown, and to stimulate an increase in protein generation.
General guidelines for nutrition before and after
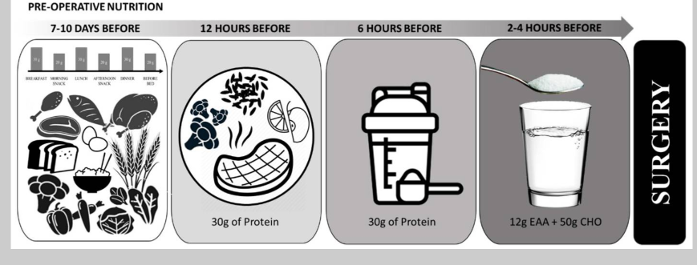
Pre-Operative Nutrition
The goal is to prepare the body for the stress of surgery, support increased metabolic demand, whilst offsetting the consequences of the breakdown of body protein. The goal of pre-operative nutrition is to ensure adequate energy stores to meet the demands of the stress state. The goal of post-operative nutrition, on the other hand, is to promote nitrogen balance, reduce the loss of lean muscle mass, and facilitate rapid healing and recovery. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
7-10 days prior to surgery - emphasise high-quality carbohydrate and protein intake to ensure optimal nourishment. To maximise glycogen stores, the sports nutrition model suggests consuming ~60% of total energy (8 g per kg body mass) per day of carbohydrate for a minimum of 3–4 days. Protein intakes of 1.2–2.0 g/kg/day, from high-quality protein sources distributed throughout the day (20–40 g of protein per meal) is recommended to help ensure protein needs are met.
6-12 hours before surgery – consume a well-rounded meal emphasising complex carbohydrates and high-quality protein.
6 hours before - begin abstaining from whole foods, but continue to consume protein and carbohydrate containing beverages, such as a protein shake, a sports drink, or chocolate milk. Since modified carbohydrate supplements rapidly empty from the stomach, consumption may sustain glucose levels for the duration of surgery.
2-4 hours before – It is suggested to ingest free form essential amino acids (EAA’s) to promote a positive protein balance. EAA’s contain all nine essential amino acids and do not require digestion.
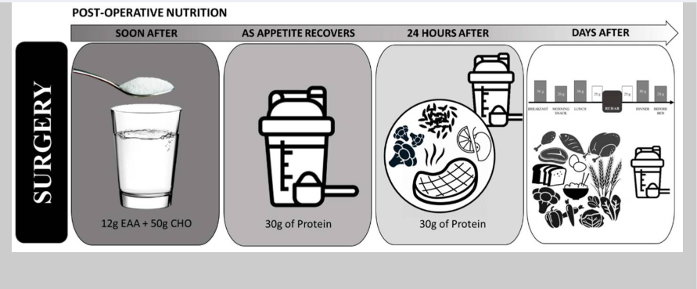
Post-Operative Nutrition
The post operative nutrition model is basically the reverse of the preoperative model.
In the early post-surgery period, patient appetite is often suppressed making consumption of solid foods difficult. During this time, free form EAA’s may help to support the immune system. Patients can transition to protein shakes and sports drinks until they are able to consume whole food sources or meals.
During the rehabilitation period, protein intakes of at least 1.6 g/kg/day and up to 2.0–3.0 g/kg/day is generally recommended. If appetite is reduced and this goal is difficult to meet then consumption of EAA’s and/or protein shakes between meals can help to optimise protein and nutrient intake.
Conclusion
In conclusion carbohydrate intake supports the increased post-surgical energy demand and wound healing. Protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Combined amino acid and glucose intake can help to mitigate muscle loss and strength, especially prior to surgery. Following surgery, free form amino acids plus supplementary dietary protein can help to support protein generation and an increase in whole-body protein. Depending on the proximity to surgery different sources of carbohydrate and protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs both pre and post-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
I frequently support clients who have either had or are going to have operations.
It is common knowledge that your nutritional status and health prior to an operation has a big impact on the outcome of surgery and your recovery post operation. It is estimated that between 24% and 65% of patients are malnourished and unfortunately this tends to increase during hospital stays. Nutritional supplementation has been shown to reduce hospitalisation costs being associated with fewer complications and shorter stays.
I have recently been researching this area for a client with impending surgery This blog is focused on protein and carbohydrate requirements both pre and post operation. I will consider micronutrient status in a future blog.
Surgery is stressful and our energy demands increase. To cope with this our sugar stores (glycogen) are rapidly burnt from the liver and muscle. This can lead to significant skeletal muscles loss and some degree of this post-surgery is inevitable. Skeletal muscle serves as the primary source of essential amino acids. If protein intake is below the requirement to sustain daily functions the body will breakdown muscle for protein. Despite this however, the hormonal stress response prevents normal protein generation. All of this is often compounded by the forced rest and immobility due to the surgery itself.
It is important to try to minimise the muscle loss and if exercise is not feasible nutritional strategies can help to mitigate this. In healthy individuals, loss of muscle tissue begins to occur in as little as 48 h of inactivity, with significant loss within five days. This is followed by loss of strength and functionality.
There some easy strategies you can implement though to help with muscle preservation and to support and accelerate healing. Carbohydrate consumption pre-operation helps to:
Support increased energy demand during the initial period and to cope with the initial inflammatory state.
Reduce muscle wastage and preserve lean body mass.
Manage the insulin resistance which is common post-surgery. Remember insulin resistance will prevent glucose entering your cells. This is important because the body will generate its own glucose (gluconeogenesis) due to the stress and it is important that the cells can absorb this.
Post-surgical amino acid supplementation has been shown to effectively reduce the turnover of whole-body protein and muscle breakdown, and to stimulate an increase in protein generation.
General guidelines for nutrition before and after surgery
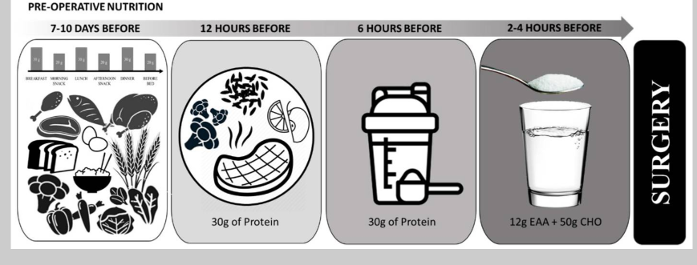
Pre-Operative Nutrition
The goal is to prepare the body for the stress of surgery, support increased metabolic demand, whilst offsetting the consequences of the breakdown of body protein. The goal of pre-operative nutrition is to ensure adequate energy stores to meet the demands of the stress state. The goal of post-operative nutrition, on the other hand, is to promote nitrogen balance, reduce the loss of lean muscle mass, and facilitate rapid healing and recovery. The guidelines given here are aimed at minimising some of the metabolic consequences of surgery, using nutritional supplementation to overcome some of the issues that whole foods would otherwise present.
7-10 days prior to surgery - emphasise high-quality carbohydrate and protein intake to ensure optimal nourishment. To maximise glycogen stores, the sports nutrition model suggests consuming ~60% of total energy (8 g per kg body mass) per day of carbohydrate for a minimum of 3–4 days. Protein intakes of 1.2–2.0 g/kg/day, from high-quality protein sources distributed throughout the day (20–40 g of protein per meal) is recommended to help ensure protein needs are met.
6-12 hours before surgery – consume a well-rounded meal emphasising complex carbohydrates and high-quality protein.
6 hours before - begin abstaining from whole foods, but continue to consume protein and carbohydrate containing beverages, such as a protein shake, a sports drink, or chocolate milk. Since modified carbohydrate supplements rapidly empty from the stomach, consumption may sustain glucose levels for the duration of surgery.
2-4 hours before – It is suggested to ingest free form essential amino acids (EAA’s) to promote a positive protein balance. EAA’s contain all nine essential amino acids and do not require digestion.
Post-Operative Nutrition
The post operative nutrition model is basically the reverse of the preoperative model.
In the early post-surgery period, patient appetite is often suppressed making consumption of solid foods difficult. During this time, free form EAA’s may help to support the immune system. Patients can transition to protein shakes and sports drinks until they are able to consume whole food sources or meals.
During the rehabilitation period, protein intakes of at least 1.6 g/kg/day and up to 2.0–3.0 g/kg/day is generally recommended. If appetite is reduced and this goal is difficult to meet then consumption of EAA’s and/or protein shakes between meals can help to optimise protein and nutrient intake.
Conclusion
In conclusion carbohydrate intake supports the increased post-surgical metabolic (energy) demand and wound healing. Protein intake supplies the amino acids needed for wound healing, immune function and preservation of muscle mass. Combined amino acid and glucose intake can help to mitigate muscle loss and strength, especially prior to surgery. Following surgery, free form amino acids plus supplementary dietary protein can help to support protein generation and an increase in whole-body protein. Depending on proximity to surgery different sources of CHO and protein can be used to maximise nutritional intake. Supplemental sources can be useful to support intake during periods when whole foods are not tolerated.
This blog is written to help inform about nutritional needs both pre and post-surgery and is based on scientific rationale. However much of this research is relatively new and further research and trials are needed to elaborate. Therefore this information does not override any medical guidelines given directly to prepare for planned surgery. These will supersede this information unless your medical team are happy to sanction otherwise.
What do Nutritional Therapists help with and how to find one?
You might be someone who gets bloated after every meal. Or someone who feels exhausted by mid-morning despite a full night’s sleep. Maybe your skin flares up regularly, or you’re dealing with unpredictable mood or energy changes.
These are just a few of the reasons people turn to nutritional therapists.
Common concerns supported by nutritional therapists include:
Digestive issues (IBS, bloating, reflux, gall bladder issues, gout etc.)
Fatigue or low energy
Pre diabetes and heart health especially cholesterol
Osteoporosis and issues with bone density
Skin conditions
Female hormonal health (PMS, perimenopause, PCOS)
Stress and mental wellbeing
Autoimmune conditions such as arthritis
Healthy ageing and preventive healthcare
Optimising athletic performance
You don’t need to be diagnosed with a condition to work with a nutritional therapist. Many clients seek support for prevention, performance, or simply to understand their bodies better.
Why People Seek Nutritional Therapy
Many people turn to nutritional therapists after trying multiple solutions—diets, supplements, or private testing—without clarity or consistent results. Others feel dismissed by standard medical care or overwhelmed by conflicting online advice.
Nutritional therapy offers a structured, evidence-informed approach to identifying patterns and making progress that lasts.
It’s ideal for anyone who:
Has symptoms that don’t have a clear medical diagnosis
Feels like they’ve tried everything but still don’t feel well
Wants to optimise health before issues become problems
Prefers natural, lifestyle-based strategies alongside medical care
How to Find a Qualified Nutritional Therapist
To ensure you’re working with a properly trained practitioner:
Look for CNHC registration – this confirms they are qualified and regulated
Check for BANT membership – this indicates high standards of ethics, education, and science-led practice
Discover the Value of Working with a BANT-Registered Nutritional Therapist
Nutritional therapists play a vital role in bridging the gap between general wellness advice and personalised healthcare. They take time to understand how your diet, genetics, environment, and lifestyle interact and use that insight to guide tailored, evidence-based recommendations that help you feel better, for longer.
Generic nutrition tips and one-size-fits-all plans can fall short. Working with a Registered Nutritional Therapist puts your individual needs at the centre. For many clients, it’s the first time their symptoms, history, and goals have been fully explored and connected into a clear plan.
This approach supports symptom improvement while also helping you reconnect with your body, increase daily energy, and take charge of your long-term wellbeing.
If you’re ready to stop guessing and start understanding what your body really needs, a Registered Nutritional Therapist could make all the difference. Please feel free to get in touch or book a call via my website.
What qualification dose a Nutritional Therapist have? Are they different from a "nutrionist"?
In the UK anyone can call themselves a “nutritionist”. The title is not legally protected so regardless of training anyone can call themselves a “nutritionist”.
However, Registered Nutritional Therapists including me are:
Fully trained in nutrition science and functional medicine
Required to register with the Complementary and Natural Healthcare Council (CNHC), a PSA-accredited regulatory body
Members of professional organisations like BANT (British Association for Nutrition and Lifestyle Medicine)
Required to follow a strict code of ethics and maintain Continuing Professional Development (CPD)
This level of regulation ensures clients are receiving safe, evidence-based advice from a qualified professional.It’s important to remember that only those registered with CNHC are recognised to deliver one-to-one clinical care.
In my case I trained with the Institute of Optimum Nutrition (ION) in London and gained a diploma (DipION, Distinction). I also did some preliminary training at the University of Westminster.
What does a 'Nutritional therapist' do?
What Does a Nutritional Therapist Do?
Have you been dealing with ongoing symptoms and feel like no one’s joining the dots? Maybe you’ve tried diets, supplements, or read endless articles online, yet nothing seems to stick. If this sounds familiar, you might be wondering if a nutritional therapist what could help.
With growing public interest in functional medicine and personalised, preventative care, nutritional therapy is gaining interest. There’s still confusion about the role, who is qualified, and how it differs from general nutrition advice. This blog explains it all.
Nutritional Therapists Offer Personalised, Evidence-Based Health Support
A nutritional therapist applies the science of nutrition and lifestyle medicine to support individuals with a wide range of health concerns. This can include digestive problems, fatigue, hormonal imbalances, immune issues, and more.
They work in a one-to-one setting, assessing each client’s health history, symptoms, diet, lifestyle, and environment to identify potential imbalances. Then they create a tailored plan that supports the body’s ability to heal and function at its best.
Nutritional therapy is:
Personalised – considering your unique biology, history, and lifestyle
Science-informed – based on the latest research in nutrition, epigenetics, and systems biology
Holistic – looking at the whole person, not isolated symptoms
The aim is not to diagnose or replace medical care, but to complement it with targeted nutritional and lifestyle recommendations.
What a Nutritional Therapy Consultation Looks Like
A consultation with a Registered Nutritional Therapist typically involves:
Detailed case history – exploring symptoms, medical history, family history, diet, lifestyle, and environment
Analysis of diet and nutrition status – sometimes supported by laboratory testing
Individualised plan – including food, supplementation, lifestyle changes, and referrals if needed
Follow-up support – adjusting the plan over time based on response and progress
This process helps the therapist and client build a picture of how different factors may be contributing to the client’s health status and how to support improvement in a structured, measurable way.
What fats can I cook with?
This blog is a reminder of which fats to use for cooking and which ones are best used cold in salad dressings. It also covers which ones to avoid.
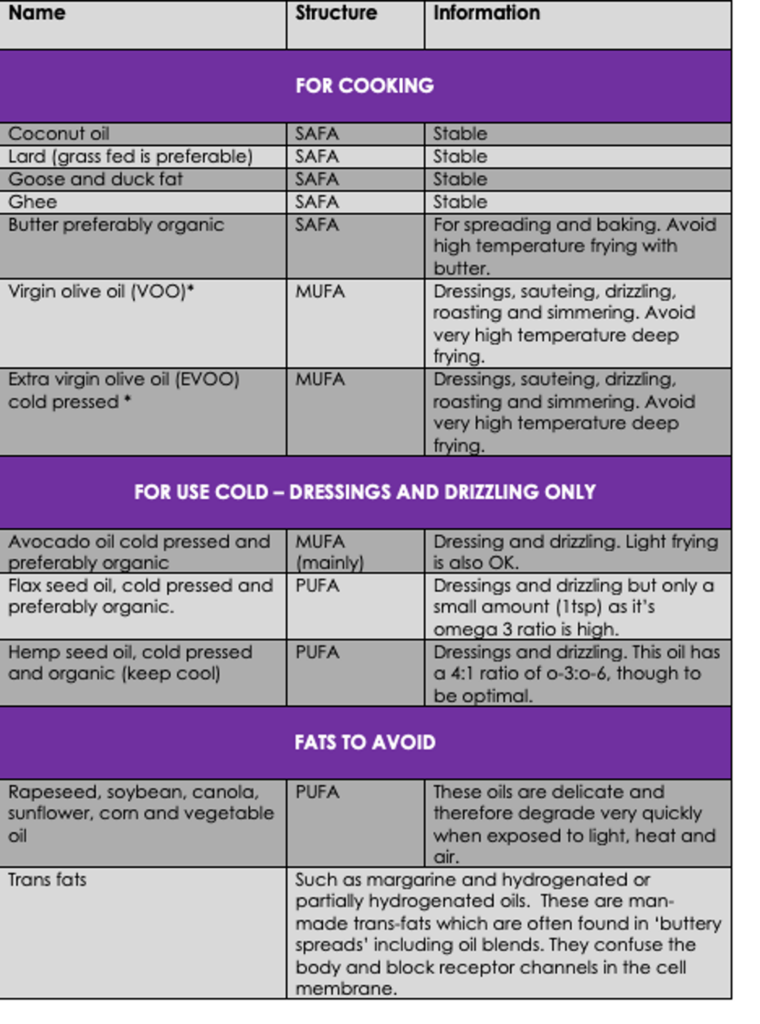
Fatty acids are classified according to the presence and number of double bonds in their carbon chain. Saturated fatty acids (SAFA) contain no double bonds, monounsaturated fatty acids (MUFA) contain one, and polyunsaturated fatty acids (PUFA) contain more than one double bond.
This table above shows the fatty acid composition of various culinary oils.
You can see from the table above that oils tend to be classified according to their largest constituent. We need to cook with oils which are stable when heated and therefore have a high smoke point. The more double bonds a fatty acid has, the more unsaturated and unstable it will be, especially when heated.
The most stable fats are solid at room temperature, so lard etc. Olive oil (virgin/extra virgin) is pressed straight from the seed or fruit without further refining. There is research to show that the phenols in unrefined olive oil protect it from degradation during cooking (Ramirez-Anaya, 2015).
Oils such as rapeseed, sunflower and vegetable are obtained by washing and crushing the seeds, and then using processes such as heating, hexane, solvents, extraction, processing, bleaching, deodorization and peroxide to maximise production volume. As these oils are highly unsaturated (many double bonds) the risk of oxidation from processing is high, either during processing or if used to cook with. Most of these oils are also much higher in omega-6 than omega-3. As our diets tend to be more deficient in omega-3, I focus on hemp and flax (small amount) which have a 4:1 and a 0.3:1 ratio respectively (o-6:o-3) to try to redress this. I also advocate cold pressed and organic versions to preserve quality and nutrient content.
The following table is a guide Whether you wish to cook with animal fats will depend on various criteria including your health and dietary preferences as well as your ability to digest and absorb fat.
Which fat to cook with and which to use for dressings and drizzles
REFS: Del Pilar Ramírez-Anaya, J. et al (2015) Phenols and the antioxidant capacity of Mediterranean vegetables prepared with extra virgin olive oil using different domestic cooking techniques. Food Chemistry Vol 188; pp. 430-438.
Do your cells need an oil change?
Today’s modern diets can often mean we eat too much or too little fat, or frequently just the wrong type. Our cell membranes consist of lots of oil aka. fat. For optimal performance they require quite a specific ratio of different types of fats, especially with regard to the essential fatty acids (EFA’s), omega 3 and 6. If these are out of sync, cells can malfunction a bit like trying to run your car on the wrong type of oil or petrol.
Cell membranes are your cells’ border control. They control what gets in and what gets out. They act as both the gatekeeper and the hostess.
Every cell in your body has a cell membrane and your body has a lot of cells. Experts think we have in the region of 30 trillion, and we want every one of these to have a healthy cell membrane. If your cell membranes are working correctly, they will let micronutrients in and waste products out. As well as supervising which molecules can enter and exit, most cell metabolism takes place in, on, or around this location. It’s like your very own production line inside you, manufacturing energy and proteins, and churning out waste products such as urea and toxins.
The next thing to understand is that their structure is critical to how well they function. We don’t want them to be too rigid or nothing will get in, or out. We also don’t want them too soft and floppy. This might allow too much in or too much out and over time this could cause multiple issues.
So how can we nourish them and maintain their structure so they can function properly? Firstly, the fat they contain needs to be eaten, as the body cannot make it. Some of these fats have special functions such as the EFA’s. There are many arguments about the correct ratio of fats to eat in the diet but researchers generally agree that we tend to be more deficient in omega 3 which is found in fish, nuts, seeds and vegetable oils.
So by now I think you get the idea that I like my clients to achieve healthy cell membranes because “the stronger our cells the more resilient our selves”.
It’s easy to check our ratios with a simple finger prick test because the concentration in our blood has been found to strongly reflect our dietary intake. The current European average for our omega 3 percentage is less than 4% but research confirms that 8% is optimum, and that this ratio is associated with a 90% reduction in risk of sudden cardiac death.
There is nothing like analytics to demonstrate to my clients (and me) that we either need to work harder on our diet or take targeted supplements to give our cells what they need to function tip top.
Here’s some simple easy changes to boost your nutrition. Check my website for recipes and to sign up to my newsletter.
Salad dressings - swop salad dressing for olive oil and lemon/apple cider vinegar (ACV) or balsamic vinegar. Mixing 1 tbsp of tahini with 6 tbsp olive oil plus 1 tbsp of lemon juice or ACV is a delicious alternative to mayonnaise. Thin with water if needed.
Crispy stuff – make your own popcorn with popcorn and olive oil plus some butter or ghee and a little salt. Alternatively roast pumpkin seeds with paprika, salt and a dash of cumin or cayenne pepper, Remember all crisps tend to contain trans-fats as they are deep fried with non-stable vegetable oils.
White for brown – this goes for rice, bread, pasta and crackers. The glycaemic index may still be high, although this is depends on the individual. But whole grain foods will retain more micro-nutrients the glycaemic response is likely to be lower, they will contain more fibre and protein and some folks do fine with them. If you soak brown rice overnight it will cook almost as quick as white.
Oats – go for steel cut or larger flakes. They are less processed and will take the body longer to breakdown, supplying a source of energy to longer.
Rice – for cauliflower rice. It’s actually very easy and it works, I’ve tried it. More fibre, more veg and less processed than rice.
Baked beans – swop your standard variety for low sugar and salt or make your own and freeze in portions.
Cow milk – for oat, rice, almond, soya or coconut. Cow milk is a major source of allergens, which are inflammatory and growth promotors. Plus many of us do not possess the lactase enzyme to digest lactose properly. It is also associated with an increased risk of osteoporosis, heart disease and auto-immunity.
Snacking on cakes, biscuits and pastries – switch to oat cakes and nut butter, nuts and seeds, one piece of fruit or a handful of berries with yogurt and hemp seeds, apple slices with a squeeze of lime juice, some nuts or seeds and a dollop of nut butter. Cakes and biscuits are full of processed ingredients and high in sugar so they will spike blood sugar and therefore insulin. They are also addictive, one is never enough.
Bread – switch to breadmaker bread and use rye flour or ancient grains such as spelt or kamut which have less gluten. You need a breadmaker that has these specialist options and it can take a while to perfect the recipe. If you are really up for the challenge switch to flax seed bread –I guarantee one slice will take you about 5 minutes to eat and you will struggle to eat a second.
Dessert – make a rule it has to be home made. I made this rule for all cakes and puddings when I first got into nutrition and as I am a lazy baker this immediately cut our consumption. Dessert, pudding, biscuits, cakes etc. need to be the exception not an expectation. But hey rules are made to be broken and a paleo crumble now and then is a great option. See my website for the recipe.
Staying alive in toxic times
This month I did a fascinating webinar with Dr Jenny Goodman, author of Staying Alive in Toxic Times, and more recently Getting Healthy in Toxic Times. Jenny is an ecological Doctor, very well respected author and rigorous researcher. The webinar was about her top 7 strategies, based on her up to date findings and research. The book will cover many more issues of course.
We all know now that everything is connected and we need to become kinder and more loving to everything, and everyone, especially nature. But how do we tackle this on an individual and daily basis? Her top three were nutrition, water filtration and cleaning up the home from indoor pollution. The issues covered in the book can cause overwhelm but as a practising Doctor she is an advocate of what I call ‘meeting people where they are’. So she includes advice regarding prioritisation and practical suggestions and ideas to tackle each area.
For example the first area ‘nutrition’ is a subject close to my heart but not everyone can afford top quality organic produce. My advice is always to buy the best you can afford. If you eat meat this is critical as animals concentrate toxicity through a process called bio-transformation. The body stores these toxins in fats to try to shield the body from harm.
There are useful strategies though such as avoiding those vegetables grown with the most pesticides such as grapes, strawberries and lettuce. You can sign up for a list of the ‘dirty dozen’ here https://mailchi.mp/pan-uk/dirty-dozen-23. There is of course also a prioritisation issue. According to Tim Spector we are one of the sickest countries in Europe but little attention is being paid to this. 33% of our income used to be spent on food, today just 8% so this is no doubt part of the problem.
Water filtration seems to be a rapidly developing area. I do have a hand-out on this if anyone is interested I am happy to send it out. She doesn’t give specific recommendations anymore because the companies themselves change what their products filter so the advice dates very quickly. What she outlines in her book are the questions which need to be checked before making a buying decision. The challenge of course is to filter out the harmful toxicity but retain or replenish the mineral content that can be lost in the process.
I was fascinated to learn that the Netherlands use physical filters and ultraviolet light to kill bacteria rather than chlorine as per the UK. This means they don’t drink ‘disinfection by- products’.
Where the home is concerned Jenny highlighted chemicals from cookware and soft furnishings, which are relatively easy to address. The most at risk are pregnant women and young children but pre conception couples should also take note here. Again there are options so if you can’t afford the organic mattress, you buy them in the summer and leave them to ‘detox’ with the windows open. Don’t paint the nursery very close to the birth etc.
I should add that there is also a lot of encouraging work being done by enterprising individuals, organisation’s and companies all of which is covered in the book. Her website if of interest is www.drjennygoodman.com.
Photo credit: Photo by Demure Storyteller on Unsplash Acera Palm known for it's ability to absorb toxic VOC compounds from the air.